
EMA has recommended granting a conditional marketing authorisation in the European Union (EU) for Abecma® (idecabtagene vicleucel), marketed by Celgene, for the treatment of adult patients with relapsed and refractory multiple myeloma (R/R MM) who have received at least three previous therapies, including an immunomodulatory agent, a proteasome inhibitor and an anti-CD38 antibody, and whose cancer has worsened since receiving the last treatment.
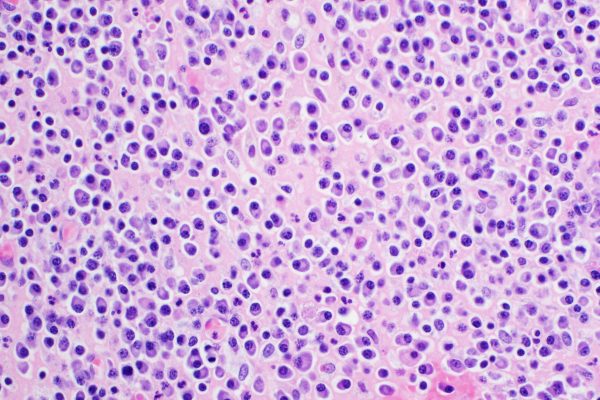
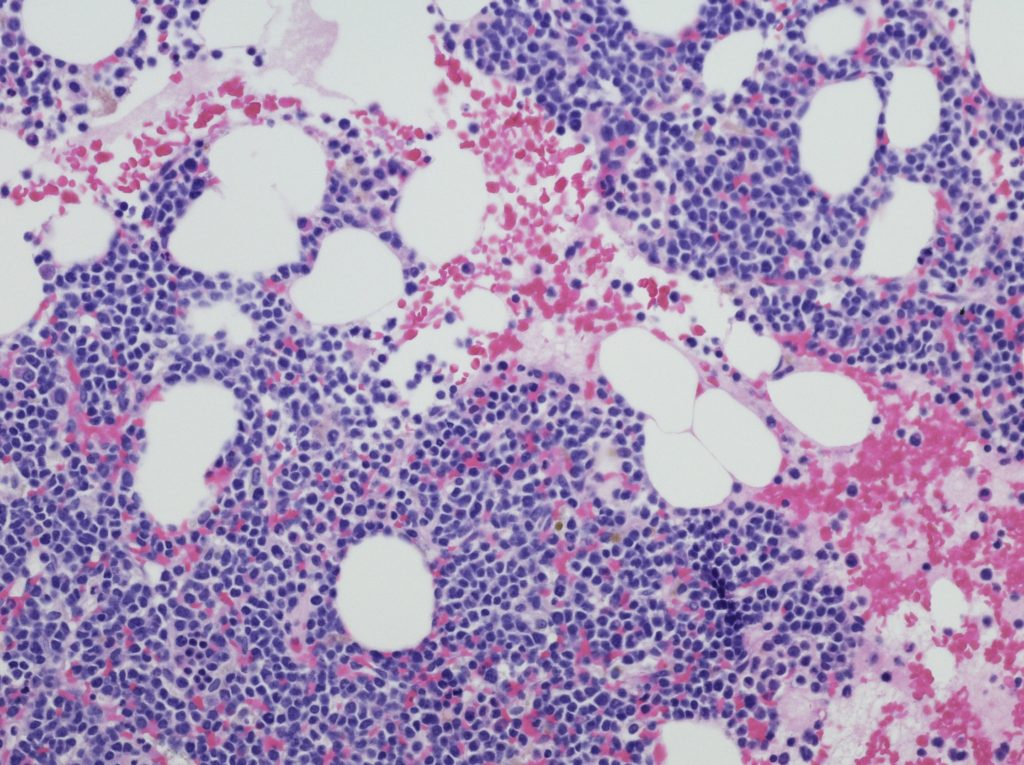
Multiple myeloma is a rare cancer of a type of white blood cell called plasma cells. Normal plasma cells are found in the bone marrow and are an important part of the immune system. Plasma cells make the antibodies that enable the body to recognise and attack germs such as viruses or bacteria. In multiple myeloma, the proliferation of plasma cells is out of control, resulting in abnormal, immature plasma cells multiplying and filling up the bone marrow. When plasma cells become cancerous, they no longer protect the body from infections and produce abnormal proteins that can cause problems affecting the kidneys, bones or blood.
Despite the development and approval of a range of new medicines for the treatment of multiple myeloma over the past few years, there are limited therapeutic options for patients who have already received three major classes of drugs (immunomodulatory agents, proteasome inhibitors and monoclonal antibodies) and no longer respond to these medicines. Therefore, new medicines are needed for patients whose disease returns after treatment.
Abecma is a genetically modified autologous chimeric antigen receptor (CAR) T-cell therapy and the first cell-based gene therapy to treat adult patients with multiple myeloma. Each dose of Abecma is created by collecting a patient’s own T-cells (i.e. white blood cells that help the body fight infections) and genetically modifying them so that they include a new gene that helps the body target and kill the myeloma cells. These modified immune cells are then infused back into the patient’s blood.
Abecma was supported through EMA’s PRIority MEdicines (PRIME) scheme, which provides early and enhanced scientific and regulatory support to medicines that have a particular potential to address patients’ unmet medical needs.
The main study on which the recommendation for a conditional marketing authorisation is based was a Phase 2, multicentre, open label, single-arm clinical trial. The study investigated the efficacy and safety of Abecma in 140 adult patients with relapsed or refractory multiple myeloma who had received at least three prior therapies, including an immunomodulatory agent, a proteasome inhibitor and an anti-CD38 antibody, and who didn’t respond to the last treatment regimen. About 67% of patients enrolled in the study responded to the treatment and maintained remission (a period without disease signs or symptoms after treatment) for about 11 months on average. Of those studied, 30% showed complete response (i.e. disappearance of signs of cancer).
The main safety concerns related to the administration of Abecma are cytokine release syndrome (CRS) (i.e. a condition causing fever, vomiting, shortness of breath, headache and low blood pressure), neurological toxicity, cytopenias (i.e. low number of cells in the blood) and infections, which can be life-threatening.
Additional efficacy and safety data are being collected through the submission of follow-up data from the main clinical trial and through an ongoing study that will compare the efficacy and safety of the medicine with standard triplet regimens in patients with relapsed and refractory multiple myeloma.
Reference

