Clinical picture
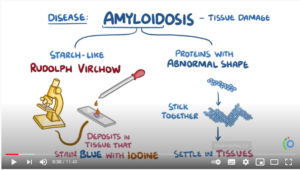
Amyloidosis is a rare and serious protein deposition disease. It includes a group of diseases in which an abnormal protein, known as amyloid fibrils, builds up in tissue or organs. As the amount of amyloid protein deposits increases in a tissue or organ, they interfere with the tissue’s or organ’s health function. Eventually, the amyloid protein deposits cause symptoms, organ failure and can be fatal.
Amyloid protein deposits may be localised to organs, such as the lung, skin, bladder and bowel or can be systemic, meaning that the deposits may be found throughout the body. Systemic amyloidosis is the most common type and although amyloidosis is not a cancer type, it may be associated with certain blood cancers like multiple myeloma.
There are about 30 different types of amyloidosis, each caused by a specific protein misfolding. Some types are genetic while others are acquired. The five most common types of systemic disease are listed here.
- Light chain (AL) amyloidosis. The amyloid proteins that build up in the tissues in this condition are known as kappa or lambda light chains. AL amyloidosis is a disorder of the plasma cells, a type of white blood cells responsible for the production of immunoglobulins or antibodies. In AL amyloidosis, the light chain proteins deposit in tissues and can damage one or more organs. The heart, kidneys, nerves and gastrointestinal system are the most common affected organs. Because AL amyloidosis is associated with the overproduction of plasma cell proteins, it is linked to multiple myeloma.
- Autoimmune (AA) amyloidosis. AA amyloidosis is also called ‘secondary amyloidosis’ or ‘inflammatory amyloidosis’. In this condition, the amyloid protein that builds up in the tissues is called the A protein. AA amyloidosis is associated with some chronic diseases, such as diabetes, tuberculosis, rheumatoid arthritis and inflammatory bowel disease. It may also be linked to ageing. AA amyloidosis can affect the spleen, liver, kidneys, adrenal glands and lymph nodes. Lymph nodes are tiny, bean-shaped organs that fight infections.
- Hereditary or familial (ATTR) amyloidosis. Hereditary amyloidosis is rare. It can be passed down from generation to generation. The proteins produced in hereditary amyloidosis may cause problems with the heart, carpal tunnel syndrome and eye abnormalities. The most common subtypes involve a protein called transthyretin (TTR).
- Acquired (non-hereditary) ATTR amyloidosis. The amyloid is formed by the normal so‑called ‘wild-type’ protein and, therefore, known as wild-type ATTR (ATTRwt) amyloidosis (formerly called senile systemic amyloidosis [SSA] because it affects people aged 80 years and older).
- Dialysis-related (Aβ2M) amyloidosis. This develops when proteins in blood are deposited in joints and tendons — causing pain, stiffness and fluid in the joints, as well as carpal tunnel syndrome. This type generally affects people on long-term dialysis.
Symptoms
The symptoms of amyloidosis can vary widely, depending on the specific organ or number of organs affected. People with amyloidosis do not always have symptoms, or the cause of a symptom may be another medical condition. All of these factors can make diagnosing amyloidosis challenging.
Symptoms of amyloidosis are usually determined by the organ or function that is affected by the protein build-up, for example:
- Reducing the kidneys’ ability to filter waste and break down proteins called nephrotic syndrome. As a result, large amounts of protein may be found in the urine, causing ‘foamy’ urine or renal insufficiency.
- Liver growth and affecting its ability to function normally. This may cause pain in the upper abdomen, swelling in the abdomen, and changes in liver enzymes that can be found using blood tests.
- Irregular heartbeats, called an arrhythmia. It may also enlarge the heart and cause poor heart function resulting in fluid build-up, an irregular heartbeat, shortness of breath, or chest pain.
- Gastrointestinal tract. Problems with the digestion and absorption of nutrients, diarrhoea or constipation, bleeding, blockages, and a thickened tongue, called macroglossia. It may also cause problems with the oesophagus, including gastro-oesophageal reflux disease (GERD).
- Thyroid gland. Goitre, a noncancerous swelling of the thyroid gland.
- Problems with breathing, including shortness of breath.
- Nervous system. Disorders of peripheral nerves causing painful paraesthesias (unusual sensations), numbness and balance difficulties, vomiting, diarrhoea, constipation, sweating, or sexual problems. Numbness, tingling, or weakness in the arms or legs may develop. This condition is known as peripheral neuropathy. Carpal tunnel syndrome may also occur.
- Especially in patients with diabetes mellitus, although it is not known if this is functionally important.
Other general symptoms of amyloidosis include:
- Fatigue, which is extreme exhaustion or tiredness.
- Unexplained weight loss.
- Anaemia, which is a low level of red blood cells.
- Weak hand grip, which may arise from carpal tunnel syndrome.
- Skin changes, such as a rash around the eyes termed “raccoon-eyes”.
- Aβ2MG amyloidosis likes to deposit in synovial tissue, causing chronic synovitis or joint pain.
- Enlargement of structures, such as an enlarged tongue in AL amyloidosis, that can lead to obstructive sleep apnoea, difficulty swallowing, and altered taste. Enlarged shoulders, results from amyloid deposition in synovial space.
- Risk of infection in AL amyloidosis because of the abnormalities in plasma cells causing a shortage of white blood cells (leukopenia), cells involved in fighting infections. Signs and symptoms of amyloidosis may not be noticed until the condition is advanced and organs are affected.
- Formation of amyloidoma, a macroscopic lump of amyloid that can cause mass effect.
Cause
Amyloidosis is caused by gene mutations that cause proteins to misfold, making them insoluble and resulting in the accumulation of these proteins in organ tissue. The proteins are at risk of misfolding as they are synthesised. Normally, these deformed proteins undergo proteolysis, which is the directed breakdown of proteins by cellular enzymes. However, the abnormal amyloid proteins are not dissolved by the body and start to aggregate. These amyloid proteins accumulate mainly in the tissue space between cells and can interfere with proper organ function.
The development of amyloidosis can be influenced by certain risk factors. A risk factor is anything that increases the chance of developing a disease. Some people with several risk factors never develop amyloidosis, while others with no known risk factors do. The cause is often unknown. The following factors may increase the risk of developing amyloidosis:
- The risk of amyloidosis increases as someone gets older. For AL amyloidosis, the majority of people are between ages 60 and 70, although earlier onset occurs.
- Amyloidosis is more common in men than in women.
- Other diseases. Having a chronic infectious or inflammatory disease, such as multiple myeloma, increases your risk of AA amyloidosis.
- Family history. Hereditary amyloidosis can run in families. This may be due to a genetic change, a mutation, that is passed down from generation to generation.
- Kidney dialysis. Not all large proteins are removed from the blood through dialysis. When on dialysis, abnormal proteins can build up in the blood and eventually be deposited in tissue. This condition is less common with modern dialysis techniques.
- Geographic origin. People of African descent appear to be at higher risk of carrying a genetic mutation associated with the type of amyloidosis that can harm the heart.
Diagnosis
Amyloidosis is often overlooked because the signs and symptoms can mimic those of more-common diseases. Diagnosis as early as possible can help prevent further organ damage. Precise diagnosis is important because treatment varies greatly, depending on your specific condition. Tests include:
- Medical history.
- Physical examination.
- Laboratory tests. Blood and urine may be analysed for abnormal protein that can indicate amyloidosis. Depending on the signs and symptoms also thyroid and liver function tests may be performed.
- Bone marrow aspiration and biopsy. These two procedures are similar and often done at the same time to examine the bone marrow. A common site for bone marrow biopsy and aspiration is the posterior iliac crest, a part of the pelvic bone located in the lower back. Bone marrow is the spongy tissue inside your bones. It has both a solid and a liquid part. A bone marrow aspiration removes a sample of the fluid with a needle. A bone marrow biopsy is the removal of a small amount of solid tissue using a needle. A pathologist then analyses the sample(s).
- The biopsy may be taken from abdominal fat, bone marrow, or an organ such as the liver or kidney. Tissue analysis can help determine the type of amyloid deposit.
- Imaging tests. To help establish the extent of the disease. Echocardiogram (EKG or ECG) may be used to assess the size and functioning of your heart.
- To create a picture of the internal organs. An ultrasound of the abdominal area may be used to look for enlarged organs.
- Genetic testing. To help determine if the amyloidosis is hereditary.
Treatment
There is no cure for amyloidosis, however treatment can help manage signs and symptoms and limit further production of amyloid protein. Specific treatments depend on the type of amyloidosis and target the source of the amyloid production.
- Chemotherapy such as cyclophosphamide and melphalan combined with dexamethasone and prednisone to stop the growth of abnormal cells that produce amyloid.
- Targeted therapy to block the growth and spread of abnormal cells while limiting damage to healthy cells. Targeted therapies include:
- Immunomodulatory drugs;
- Monoclonal antibodies;
- Proteasome inhibitors
- Surgery may include organ transplantation of the liver, kidney and heart.
- Autologous blood stem cell transplant (ASCT) or bone marrow transplantation in which the plasma cells in the bone marrow that produce amyloid protein are first destroyed by high doses of chemotherapy and then replaced by highly specialized cells, called hematopoietic stem cells, that develop into healthy bone marrow.
- Anti-inflammatory medication or diuretics to target the underlying condition.
- Nutritional adjustments such as a low-salt diet for patients with gastrointestinal amyloidosis.
- Support stockings may be recommended for patients with leg swelling.
- Laser treatment of localized amyloidosis. Pulsed dye laser (PDL) in nodular amyloidosis, and the YAG laser in macular amyloidosis.
Additional information
Related articles

Clinical picture

Symptoms

Cause

Diagnosis

Treatment

Patient organisations

Links