Journal issues>Issue 7, November 2021>PARTNER-project: A model and tools to support shared decision making in relapsed/refractory multiple myeloma (RRMM) treatment
PARTNER-project: A model and tools to support shared decision making in relapsed/refractory multiple myeloma (RRMM) treatment
Treatment options for multiple myeloma have increased substantially. To find the best therapy for each individual patient, patient preferences should be taken into account whenever a decision regarding relapsed/refractory multiple myeloma (RRMM) treatment has to be made. Shared decision-making (SDM) is one of the keys to person-centred care. Previous research, using semi-structured interviews, investigated the experiences and preferences of Belgian RRMM patients and their carers regarding involvement in decisions related to treatments. The aim of this part of the PARTNER-project was to develop a model and tools to support the implementation of SDM in RRMM treatment.
The practice model for SDM and the proof of concepts of the tools were developed using a 2-phase co-design approach. First, results from the interviews were combined with data from the literature to draft the model and tools. In the second phase, meetings with expert panels were set up to discuss the model and tools and to adapt them according to the feedback.
The PARTNER model for SDM in RRMM that has been developed as part of this project is a conceptual framework, describing essential elements in the decision-making process. Four tools were designed to convert the model into practice. It concerns 1) a question prompt list, to be used by patients to prepare for consultations with clinicians; 2) knowledge clips for patients and healthcare professionals (HCPs) to enhance the understanding of the SDM concept; 3) a conversation starter, aimed to open the dialogue among HCPs about organising and implementing SDM; and 4) a conversation tool, which is a hands-on step-by-step guide for conversations about treatment options between HCPs and RRMM patients. Additionally, suggestions on dissemination strategies were formulated.
Efforts were made to enhance a fit of the PARTNER model and tools into the Belgian RRMM setting. For some of the tools, evidence was provided on the improvement of the decision-making process, but none of the tools were yet tested. Further research should focus on pilot testing and evaluating the tools regarding their impact and feasibility to support SDM.
(BELG J HEMATOL 2021;12(7):305–17)
Press play button to have the text read to you.
SUMMARY
Treatment options for multiple myeloma have increased substantially. To find the best therapy for each individual patient, patient preferences should be taken into account whenever a decision regarding relapsed/refractory multiple myeloma (RRMM) treatment has to be made. Shared decision-making (SDM) is one of the keys to person-centred care. Previous research, using semi-structured interviews, investigated the experiences and preferences of Belgian RRMM patients and their carers regarding involvement in decisions related to treatments. The aim of this part of the PARTNER-project was to develop a model and tools to support the implementation of SDM in RRMM treatment.
The practice model for SDM and the proof of concepts of the tools were developed using a 2-phase co-design approach. First, results from the interviews were combined with data from the literature to draft the model and tools. In the second phase, meetings with expert panels were set up to discuss the model and tools and to adapt them according to the feedback.
The PARTNER model for SDM in RRMM that has been developed as part of this project is a conceptual framework, describing essential elements in the decision-making process. Four tools were designed to convert the model into practice. It concerns 1) a question prompt list, to be used by patients to prepare for consultations with clinicians; 2) knowledge clips for patients and healthcare professionals (HCPs) to enhance the understanding of the SDM concept; 3) a conversation starter, aimed to open the dialogue among HCPs about organising and implementing SDM; and 4) a conversation tool, which is a hands-on step-by-step guide for conversations about treatment options between HCPs and RRMM patients. Additionally, suggestions on dissemination strategies were formulated.
Efforts were made to enhance a fit of the PARTNER model and tools into the Belgian RRMM setting. For some of the tools, evidence was provided on the improvement of the decision-making process, but none of the tools were yet tested. Further research should focus on pilot testing and evaluating the tools regarding their impact and feasibility to support SDM.
(BELG J HEMATOL 2021;12(7):305–17)
INTRODUCTION
Over the past decade, treatment options for multiple myeloma (MM) have increased remarkably, and many more drugs are in the pipeline.1–3 As there is no single and uniform guideline on which drugs to use in which circumstances, the selection of optimal anti-MM treatment is difficult.4 Ideally, patients are involved in the choice of the treatment, but this can be overwhelming for patients and informal caregivers. Clinicians may also feel uncomfortable in discussing the options.5 The complexity of the treatment decision-making process in the haematological setting not only requires critical review by the clinician but also a two-way dialogue with the patient regarding treatment goals, values, preferences, and needs of the patient.1,6 Previous studies, targeting individuals newly diagnosed with MM, showed an increasing patient need for information regarding treatment and for disease knowledge, specific for those who are diagnosed with MM at a younger age.7–9 These studies indicate there is a need among MM patients for disease- and treatment related information and a willingness to participate in cancer treatment decision-making.10
Recently, the American Society of Clinical Oncology (ASCO) released a consensus guideline that recommends clinicians to provide information oriented to the concerns and preferences of the patient, and to consider patients’ treatment goals.11 Enhancing shared decision making (SDM) in the treatment of relapsed/refractory multiple myeloma (RRMM) may provide an impactful opportunity to enhance person-centred care.6,12 Elwyn et al. defined SDM as: “An approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences”.13 The aim of SDM is the collectively agreement of the healthcare professional (HCP) and the patient on a healthcare choice that is based on the best available research evidence, clinical expertise, and the values of the informed patient.14–18 Today, it is unclear how SDM is performed in the RRMM setting, and how patients with RRMM experience decisions regarding their treatment.
In the first part of the PARTNER project, a prospective and multicentric observational study on SDM in RRMM patients, we examined current practice regarding patient and informal caregivers’ involvement in decisions related to medication. To get insight into patients’ experiences and expected level of involvement, semi-structured interviews with RRMM patients and their informal caregivers were conducted. Besides, interviews with HCPs (haematologists, nurses, onco-coaches and pharmacists) have been performed to get insight into HCPs’ experiences and perceived opportunities for patient and carer involvement. The aim of the second part of the project was to develop a model and tools to support the implementation of SDM in RRMM treatment, using a co-design approach.
DEVELOPMENT OF THE MODEL AND THE TOOLS
The practice model for SDM in RRMM treatment and the proof of concepts of the tools were developed using a 2-phase co-design approach.
In phase 1, the research team combined the results from the interviews with data from the literature to develop a first draft of a practice model for SDM and tools to support practice.
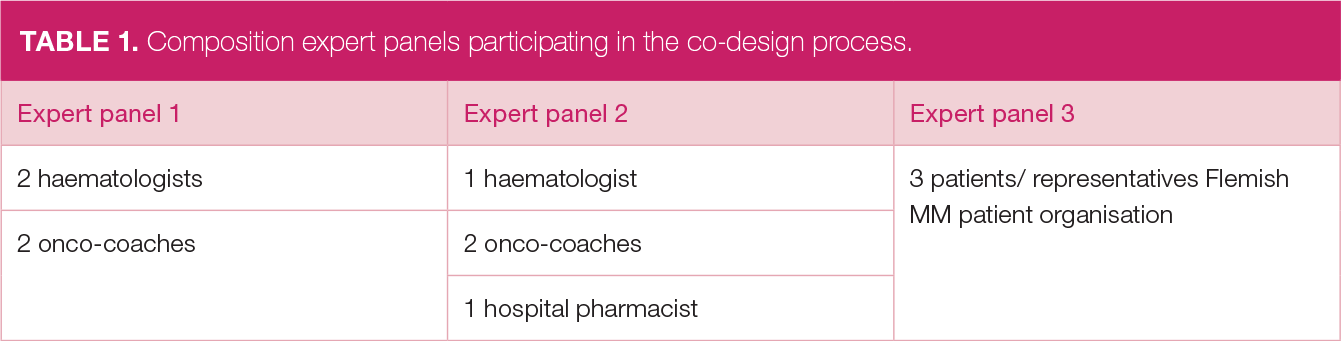
In phase 2, three meetings with expert panels were set up to discuss the model and the tools. Table 1 gives an overview of the expert panels: two panels with HCPs (haematologists, onco-coaches, hospital pharmacists) from different hospitals in Flanders and one with representatives of the Flemish MM patient organisation.
TABLE 1. Composition expert panels participating in the co-design process.
Hospitals participating in the co-design process were also included in the first part of the PARTNER project (interviews). Participants of the co-creation meeting signed an informed consent in advance. Meetings were audiotaped to facilitate the processing of the data.
The co-design meetings started with presenting the results of the interviews of the first part of the PARTNER project. Then the draft versions of the model and tools were shown one by one, with breaks in between to start the discussion. Experts were explicitly asked to give their comments, and to make suggestions for adaptations. The model and tools were then adapted according to these suggestions, in an iterative process.
At the end of this process, a meeting with an HCP (haematologist) affiliated to a hospital in Wallonia was organised to validate the results that were obtained from the co-design process with HCPs from Flemish hospitals. A similar meeting was set up with a representative of the Walloon MM patient organisation.
RESULTS
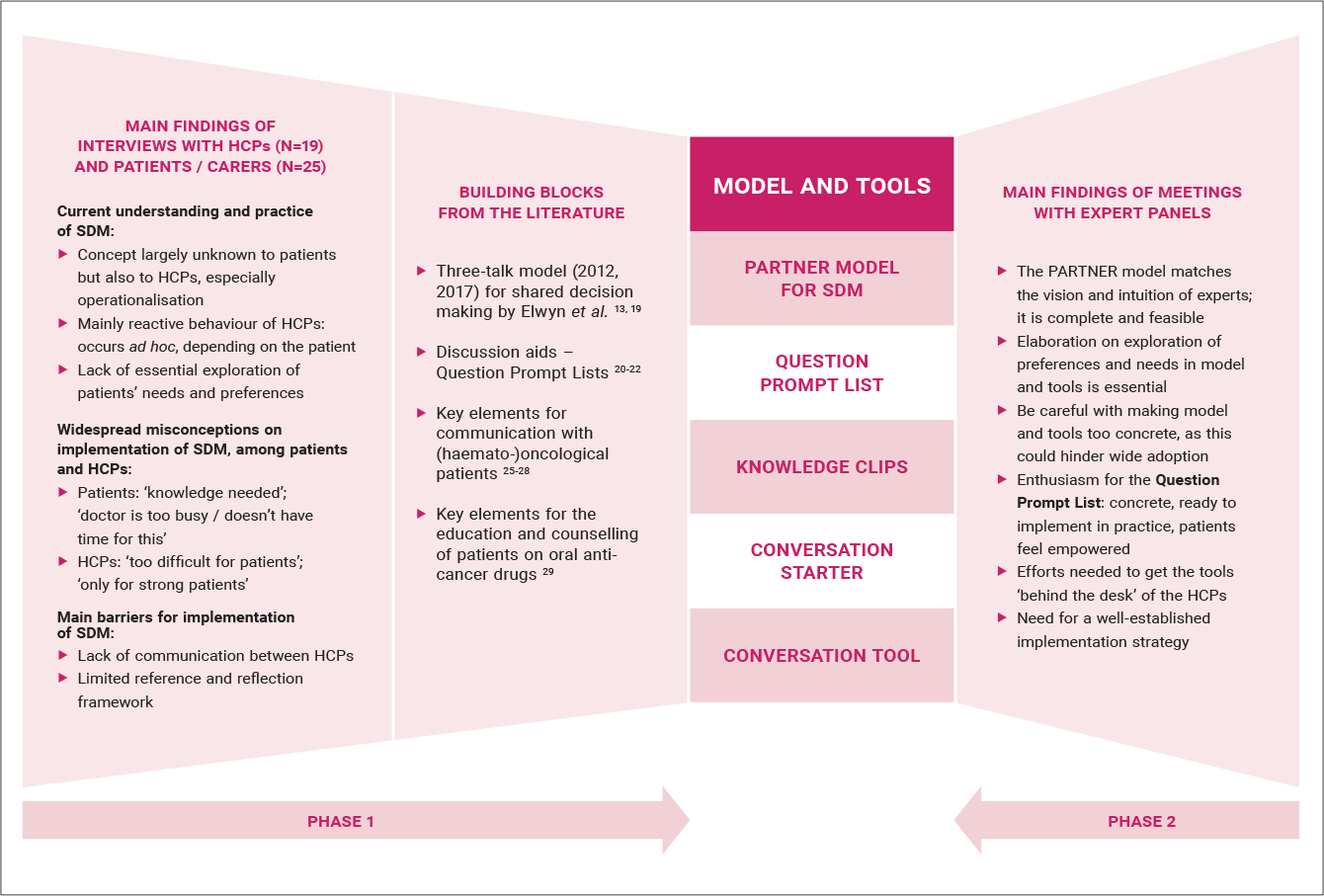
A full overview of the 2-phase co-design development of the PARTNER model for SDM in RRMM treatment and tools can be found in Figure 1.
FIGURE 1. Summary of the 2-phase co-design development of the PARTNER model and tools.
This figure represents the main findings of the interviews that were combined with building blocks from the literature (left panels) to construct the draft versions of the PARTNER model for SDM in RRMM treatment, and the tools. The right panel shows the main findings of the meetings with the expert panels that provided evidence for modifications of the model and the tools.
In what follows, we describe for the model and each of the tools the aims and characteristics, the findings from the interviews that demonstrated the need for the model / tools, evidence from literature that was used to construct the model/tools, and data from the co-design process with experts that were used to finalise the materials.
Partner model for SDM in RRMM treatment
The PARTNER model for SDM in RRMM is a conceptual framework, describing essential elements in the decision-making process regarding treatment. The aim of this model is to enhance the understanding of how SDM can be practiced, to support the development of care that enables SDM, and to avoid ad hoc and reactive behaviour of HCPs. This model functions as an elicitation of the central idea of SDM, the fundament for tools to implement this approach in practice. Once HCPs are familiar with the central idea of the model, they can adopt the tools that will assist them in converting the PARTNER model for SDM into practice.
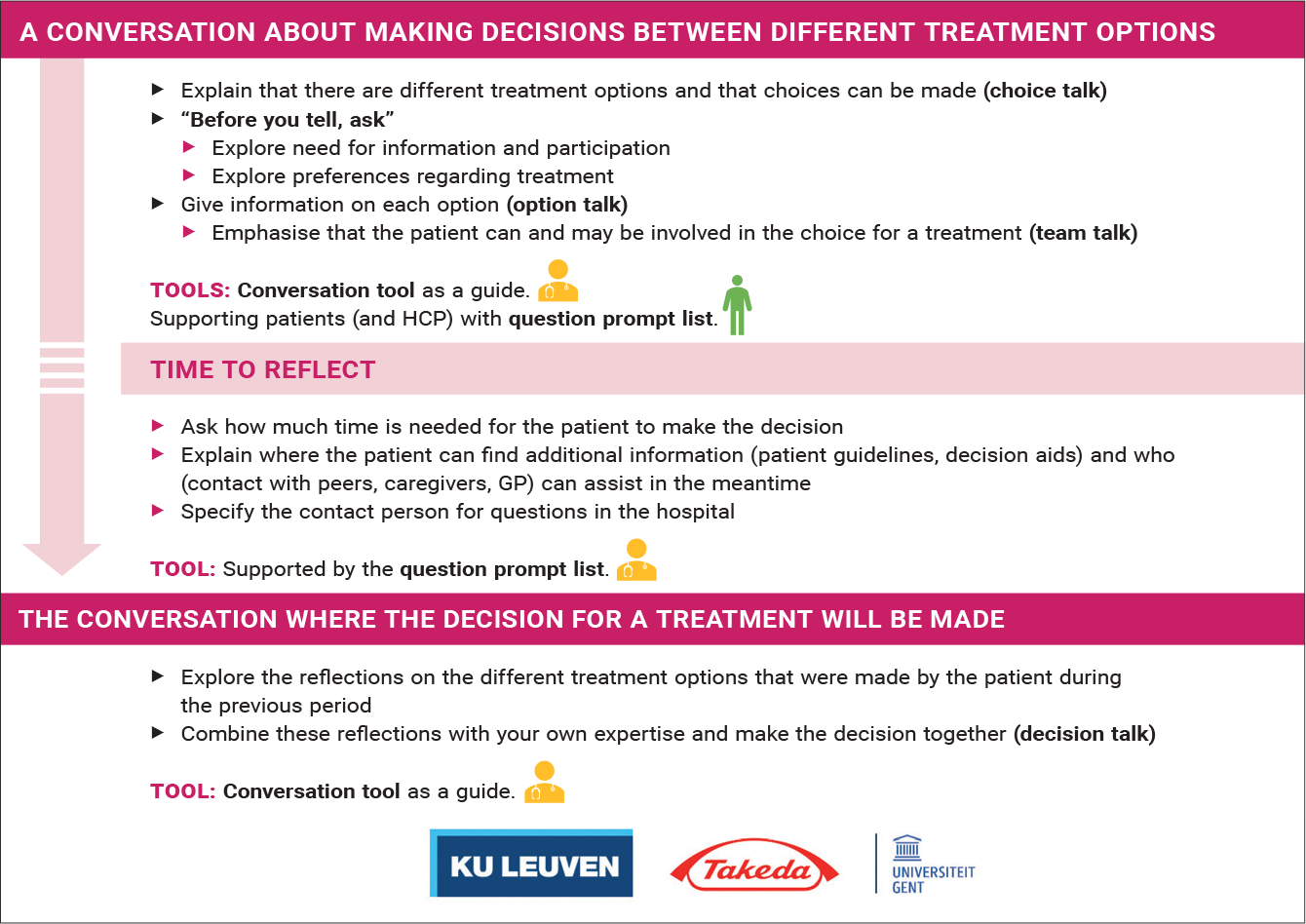
During the interviews, we noticed that HCPs in the field of RRMM need a clear guidance that mirrors the decision-making pathway. Therefore, a linear model was developed. The theoretical basis of this model can be found in a combination of the 2012 and the 2017 three-talk model developed by Elwyn et al.13,19 In the 2012 model, they distinguished the following parts: ‘choice talk’, ‘option talk’ and ‘decision talk’. A revised version was made in 2017: among other modifications, the term ‘choice talk’ was replaced with ‘team talk’. Although reasonable arguments were formulated for this modification, we agreed that both terms (and in fact both steps) are relevant for the RRMM setting.19 In the interviews, it became clear that patients and caregivers often do not have insight in the possibility to make choices between multiple treatment options. Based on this finding, the research team concluded to use the term ‘choice talk’ to describe the first step in the SDM process. Besides, patients often interpreted participating in a decision as being faced with the task to make a decision on their own. For this reason, it felt important to also retain the term ‘team talk’, and to fully integrate talking about the fact that patients are considered part of the team deciding on the treatment options, in the model. The model can be found in Figure 2.
HCPs in the expert panels stated that the model matches their vision and intuition; they called it ‘complete’ and ‘ feasible’. While this model seems to visualise their ideal practice, they acknowledged that current practice is not always according to the model. HCPs emphasised that they are especially struggling with exploring needs/preferences/expectations, before they explain options. This confirmed our results from the interviews. We adapted the model in that way, which we highlighted and further elaborated on the exploration phase. Besides, HCPs advised to be careful with making the model too concrete, as it could hinder a wide adoption.
Patients commented that ‘time to reflect’ can be a torment and will not be necessary for each patient or decision. As the interviews with patients and informal caregivers showed that for some patients ‘time to reflect’ is needed to make an informed and shared decision, and that this is often forgotten by HCPs, we concluded that ‘time to reflect’ should be included as a theme in the model, but we visualised it as less mandatory. A sentence was added to the model, to stimulate HCPs to ask how much time the patient would need to make an informed decision, and to come back for the ‘decision talk’.
Partner tools to support SDM
Four tools were developed to support SDM in practice. It concerns 1) a question prompt list, to be used by patients to prepare for consultations with clinicians, 2) knowledge clips for patients and HCPs to enhance the understanding of the SDM concept, 3) a conversation starter, aimed to open the dialogue among HCPs about organising and implementing SDM, and (4) a conversation tool, which is a hands-on step-by-step guide for conversations about treatment options between HCPs and RRMM patients.
Question Prompt List
Since patients clearly mentioned to experience a threshold to ask questions to clinicians, a question prompt list (QPL) was built. This is a list of questions patients can ask during the decision-making process. This tool was designed based on the topics that were addressed in the interviews, combined with topics from previous or generic QPLs and is aimed to trigger a two-way dialogue during decision-making consultations.20–22 In previous studies with QPLs, it was found that patients never ask literal questions from the list, but adjust them to their circumstances.23 For this reason, additional space was provided on the QPL to make notes.
When presenting the QPL to the expert panels, their feedback on this tool was very positive. HCPs found it a concrete tool, which they could immediately implement in practice. Patients mentioned that a QPL would really help them. First, they felt that a QPL would support them, and make them more empowered. It would help them to open the dialogue when they have a tool to refer to. They also stated that the questions were relevant and the list was complete. This was confirmed by the HCPs. Their advice was to not address which HCPs need to answer which questions, and to leave it up to the hospitals to adjust this to their specific setting. Patients preferred to have a paper-version over a digital one, although availability of a downloadable form on the websites of hospitals and patient organisations would be welcome.
Instructional avatar movies on SDM, called ‘knowledge-clips’, were suggested to make HCPs and patients familiar with the concept.
During the interviews, it became clear that SDM is a completely unknown concept to RRMM patients. Misidentification of the concept made it sometimes difficult to answer the questions posed in the interviews with patients in the first part of this research project. A short movie could act as a revelation for patients, to show them what SDM is about and that they can play a role in the decision-making process. Having watched a video on SDM might help patients to take up their role, when SDM is introduced in their treatment.
Patients in the expert panel acknowledged that they prefer a video over a text to introduce the concept of SDM. They considered it more accessible and easier to reach all groups of patients. To enhance recognisability, patients suggested including quotes from peers. HCPs suggested running the movie on LCD screens in waiting rooms, to share it on websites of patient organisations and hospitals, and to make it accessible with a QR-code on leaflets for patients. Since the concept of SDM is not only unknown to patients but also to HCPs (especially its operationalisation), instructional movies for HCPs were suggested as well. The idea was in fact to develop two knowledge-clips for HCPs: a first one elaborating on the concept of SDM (what it is and why both patients and HCPs would benefit from it), and a second one on implementing SDM, including a presentation of the model and tools developed as part of the PARTNER project.
The feedback on knowledge-clips for HCPs was less straightforward than the feedback on a short movie for patients. Some experts thought it would certainly be a good idea, while others were hesitating, especially regarding the uptake in practice. It became clear, however, that efforts would be needed to make the materials known to the target group, and that a combination of approaches might be essential.
Although the idea of making knowledge clips was received with some enthusiasm, caution was advocated in its implementation, in order to avoid excessive expectations in patients. Therefore, it was thought that the further development of these tools would be better part of a larger implementation project.
Conversation Starter
The conversation starter is a guide and a presentation kit to support an open dialogue among HCPs about organising and implementing SDM. Given the current lack of framework and vision on the concept of SDM and its implementation in practice, the conversation starter is thought to contribute to the development of a more structured approach for SDM in RRMM care.
The conversation starter could be used to structure and support interdisciplinary meetings among HCPs on the level of the care unit. During these meetings, HCPs could reflect on the current decision-making process. This reflection, combined with the knowledge gained from the knowledge-clips and PARTNER model for SDM in RRMM, would allow to open the discussion and to have an in-depth dialogue on the topic within the team or care unit. The slide-kit would further support making concrete agreements on how SDM, the model and tools could be implemented in the hospital.
When introducing a preliminary version of this tool to the expert panels, different reactions came up. Some HCPs mentioned that talking about organisation of care and patient consultations within the team or care unit is difficult, and that a meeting on how to organise care is currently not happening in most hospitals. Therefore, HCPs advised to introduce and moderate such meetings by external moderators, who would be able to take up a more neutral role, and to stimulate the dialogue as well as coming to concrete agreements. During the discussions, it became also clear that patients are currently not involved in the development of care pathways in hospitals. However, given the topic of the proposed meetings, it would be a good idea to invite patients as well in order to discuss the concrete implementation of SDM. Some HCPs and patients of the expert panels showed openness towards this idea, but thought it would only work as part of a larger implementation project.
Conversation Tools
The interviews showed that, within current care, the exploration of preferences and needs of patients is rather limited. Clinicians also struggle to have an open discussion with patients on the treatment options. These findings are in line with findings from previous research on physician communication styles in haematological cancers.24
The conversation tool therefore concerns a hands-on systematic guide for conversations about treatment options between HCPs and RRMM patients, including examples of key questions and phrases, and suggestions for an empathic and clear approach. Two different conversation tools were developed to cover both parts of the PARTNER model for SDM: a conversation tool for the choice, option and team talk, and a conversation tool for the decision talk. Fundaments for these tools were found in the optimisation opportunities that were suggested in the interviews, and in evidence from previous research on communication with (haemato-)oncological patients and care goals.13,19,25–29 HCPs in the expert panel appreciated the format and content of the conversation tools. However, they highlighted the difficulties of implementing this kind of tools in practice. Suggestions were made to print it on a desk coaster or make a pocket format. The tool should remind them on a regular basis of all essential steps in the process.
The conversation tools do not address which HCPs should be involved in the different parts of the conversations, as it became clear in the interviews that the organisation of care varies among hospitals, and that decisions on this aspect should left open to the hospitals. However, we recommend considering the involvement of the onco-coach in the option talk, since patients seem to appreciate their communication skills and approachable contact. This was also suggested by the patients’ expert panel.
While reviewing the literature as part of this project, it became clear that there is no single solution to implement SDM, and that it is important to work tailored to the envisaged setting.17 Therefore, the PARTNER model and tools have been developed in co-design with all stakeholders: starting from interviews with a high number of patients, carers and HCPs affiliated to different Belgian hospitals, and integrating feedback from diverse experts. By using this approach, we were able to enhance a fit of the developed model and tools into the Belgian RRMM setting. Moreover, the model and the tools are intertwined, and focus on different aspects that are essential for the implementation of SDM. Limiting the adoption to one of the tools might not lead to the desired shared decision-making process.
During the co-design process, it became clear that some participants were very enthusiastic about the different tools, and were hoping for a rapid implementation in practice. However, the model and the tools have not yet been tested in practice. We learned during the co-design process that simply diffusing the model and the tools into practice will probably not lead to sustainable changes; this has been clearly confirmed in previous implementation research. 30 The first focus should therefore be on pilot-testing and evaluating the tools with regard to the impact on patient / caregiver involvement in decisions related to treatment and the perceived impact and feasibility of the tools to support SDM in practice. To make an evaluation of the integrated model and tools, the FAME framework could be used.31 Next; efforts will need to be made on communication about the model and tools to increase awareness among stakeholders, and to obtain a sustainable implementation in practice. Therefore, we believe a larger implementation project is needed.
For some of the tools, there is clear evidence that they might improve the decision-making process, as shown by previous research in other groups of oncological patients. A cohort study of terminally ill cancer patients showed that patients who were provided with a QPL asked more questions and reported less unmet needs.32 Besides, the introduction of a QPL in oncology consultations led to an increase of expressed preferences.33 In a systematic review on the effects of a QPL in oncological settings, Keinki et al. concluded that QPLs are inexpensive tools that influence communicative processes positively.34 Moreover, introduction of a QPL did not increase the consultation time.35,36 Based on the results of the co-design meetings, we are convinced that it will not suffice to just distribute the list to patients; the QPL should be implemented in the consultations and HCPs need to refer to the list proactively. This advice is supported by previous research of Brown et al., who concluded that a QPL only improved information recall and decreased anxiety levels when HCPs specifically addressed the QPL.37 The same study observed a significantly shorter consultation length when a QPL was actively endorsed by an HCP.
The idea of using videos to inform and educate patients in SDM was previously used in other oncology settings: instructional video’s showed positive results in SDM on prostate antigen-testing.38–40 Besides, multidimensional interventions aiming to improve SDM often include videos as patient education material.41 To our knowledge, less evidence can be found on the use of instructional videos to educate HCPs on SDM.
Chhabra et al. confirmed our finding from the interviews that HCPs tend to ‘broadcast’ information on different treatment options. This one-directional manner of communication and the overabundance of information seemed to increase anxious emotions and confusion in patients.24 The authors concluded that HCPs who apply a more inviting communication style, encourage patient participation. The conversation tools that we developed are specifically designed to meet that need, and to enhance bi-directional communication in conversations related to making treatment decisions.
To our knowledge, there are no previous initiatives which aim to support an open dialogue among HCPs about organising and implementing SDM, which is the purpose of the conversation starter that we developed. However, there is ample evidence that changes in organising care are only successful if they are discussed with all relevant HCPs.42
CONCLUSION
Using a rigorous co-design approach with integration of all stakeholders, we developed the PARTNER model for SDM in RRMM treatment and tools to support SDM in practice. For some tools, there is clear evidence that they will improve the decision-making process. Before the desired impact can be measured and a large implementation can be strived for, further research should focus on pilot testing and evaluating the tools regarding their impact and feasibility to support shared decision-making.
KEY MESSAGES FOR CLINICAL PRACTICE
The American Society of Clinical Oncology (ASCO) released a consensus guideline that recommends clinicians to provide information oriented to the concerns and preferences of the patient, and to consider patients’ treatment goals.
Results from interviews with patients, carers and HCPs have shown that the concept of SDM is largely unknown: it only happens ad hoc, depending on the patient.
Patients and carers would benefit from open conversations with active listening and in-depth exploration of preferences and the need for involvement, when faced with the task of making treatment-decisions.
The PARTNER model describes all essential elements of the shared decision-making process for RRMM treatment.
The Question Prompt List, Conversation Tool, Conversation Starter and Knowledge Clips are tools developed to support SDM in practice.
References
1. Wilke T, et al. Treatment of relapsed refractory multiple myeloma: which new PI-based combination treatments do patients prefer? Patient Prefer Adherence. 2018;12:2387–96. 2. Cook G, et al. A question of class: Treatment options for patients with relapsed and/or refractory multiple myeloma. Crit Rev Oncol Hematol. 2018;121:74–89. 3. Moreau P, et al. Global Approaches in Myeloma: Critical Trials That May Change Practice. Am Soc Clin Oncol Educ Book. 2018;38:656–61. 4. Kumar SK, et al. NCCN Guidelines Insights: Multiple Myeloma, Version 3.2018. J Natl Compr Canc Netw. 2018;16(1):11–20. 5. Covvey JR, et al. Barriers and facilitators to shared decision-making in oncology: a systematic review of the literature. Support Care Cancer. 2019;27(5):1613–37. 6. LeBlanc TW, et al. Review of the patient-centred communication landscape in multiple myeloma and other hematologic malignancies. Patient Educ Couns. 2019;102(9):1602–12. 7. Tariman JD, et al. Top Information Need Priorities of Older Adults Newly Diagnosed With Active Myeloma. J Adv Pract Oncol. 2015;6(1):14–21. 8. Kane HL, et al. Implementing and evaluating shared decision making in oncology practice. CA Cancer J Clin. 2014;64(6):377–88. 9. Rood JA, et al. Perceived need for information among patients with a haematological malignancy: associations with information satisfaction and treatment decision-making preferences. Hematol Oncol. 2015;33(2):85–98. 10. Tariman JD, et al. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–51. 11. Gilligan T, et al. Patient-Clinician Communication: American Society of Clinical Oncology Consensus Guideline. J Clin Oncol. 2017;35(31):3618–32. 12. Légaré F, et al. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff (Millwood). 2013;32(2):276–84. 13. Elwyn G, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–7. 14. Charles C, et al. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–92. 15. Legare F, et al. Interventions for improving the adoption of shared decision making by healthcare professionals. Cochrane Database Syst Rev. 2014(9): CD006732. 16. Weston WW. Informed and shared decision-making: the crux of patient-centred care. CMAJ. 2001;165(4):438–9. 17. Barratt A. Evidence Based Medicine and Shared Decision Making: the challenge of getting both evidence and preferences into health care. Patient Educ Couns. 2008;73(3):407–12. 18. Vandvik PO, et al. Creating clinical practice guidelines we can trust, use, and share: a new era is imminent. Chest. 2013;144(2):381–9. 19. Elwyn G, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. 20. McLawhorn VC, et al. Integrating a Question Prompt List on an Inpatient Oncology Unit to Increase Prognostic Awareness. Clin J Oncol Nurs. 2016;20(4):385–90. 21. kanker.nl. Vragen uit de app Gesprekshulp bij kanker [Available from: https://www.kanker.nl/gesprekshulp/vragen-voor-het-gesprek]. 22. Van Hecke A, et al. Het Digitaal Onco Platform (DOP): op weg naar verdieping en verbreding. Optimalisatie en implementatie van het eHealth platform voor kankerpatiënten. Stichting Tegen Kanker, Social Grant. 2015. 23. Brandes K, et al. Advanced cancer patients’ and caregivers’ use of a Question Prompt List. Patient Educ Couns. 2014;97(1):30–7. 24. Chhabra KR, et al. Physician communication styles in initial consultations for hematological cancer. Patient Educ Couns. 2013;93(3):573–8. 25. Paladino J, et al. Patient and clinician experience of a serious illness conversation guide in oncology: A descriptive analysis. Cancer Medicine. 2020; 9(13):4550–60. 26. Bernacki RE, et al. Communication About Serious Illness Care Goals. JAMA Internal Medicine. 2014;174(12):1994. 27. Morgans AK,et al. Confronting Therapeutic Failure: A Conversation Guide. The Oncologist. 2015;20(8):946–51. 28. Leblanc TW, et al. Review of the patient-centred communication landscape in multiple myeloma and other hematologic malignancies. Patient Educ Couns. 2019;102(9):1602–12. 29. Kinnaer L-M, et al. Key elements for the education and counselling of patients treated with oral anticancer drugs. Eur J Oncol Nurs. 2019;41:173–94. 30. Lomas J. Diffusion, dissemination, and implementation: who should do what? Ann N Y Acad Sci. 1993;703:226–35; discussion 35–7. 31. Pearson A, Wiechula R, Court A, et al. The JBI model of evidence-based healthcare. Int J Evid Based Healthc. 2005;3(8):207–15. 32. Clayton JM, et al. Randomized controlled trial of a prompt list to help advanced cancer patients and their caregivers to ask questions about prognosis and end-of-life care. J Clin Oncol. 2007;25(6):715–23. 33. Rodenbach RA, et al. Promoting End-of-Life Discussions in Advanced Cancer: Effects of Patient Coaching and Question Prompt Lists. J Clin Oncol. 2017;35(8):842–51. 34. Keinki C, et al. Effect of question prompt lists for cancer patients on communication and mental health outcomes—A systematic review. Patient Educ Couns. 2021. 35. Bruera E, et al. Breast cancer patient perception of the helpfulness of a prompt sheet versus a general information sheet during outpatient consultation: a randomized, controlled trial. J Pain Symptom Manage. 2003;25(5):412–9. 36. Smets EM, et al. Addressing patients’ information needs: a first evaluation of a question prompt sheet in the pretreatment consultation for patients with esophageal cancer. Dis Esophagus. 2012;25(6):512–9. 37. Brown RF, et al. Promoting patient participation and shortening cancer consultations: a randomised trial. Br J Cancer. 2001;85(9):1273–9. 38. Onel E, et al. Assessment of the Feasibility and Impact of Shared Decision Making in Prostate Cancer. Urology. 1998;51(1):63–6. 39. Ross L, et al. Applicability of a video intervention to increase informed decision making for prostate-specific antigen testing. J Natl Med Assoc.2010;102(3):228–36. 40. Frosch DL, et al. A randomized controlled trial comparing internet and video to facilitate patient education for men considering the prostate specific antigen test. J Gen Intern Med. 2003;18(10):781–7. 41. Tai-Seale M, et al. Enhancing Shared Decision Making Through Carefully Designed Interventions That Target Patient And Provider Behavior. Health Aff (Millwood). 2016;35(4):605–12. 42. Kinnaer LM, et al. Collaborative network to take responsibility for oral anticancer therapy (CONTACT): Study-protocol investigating the impact of a care pathway. J Adv Nurs. 2019;75(12):3726–39.
About authors
Please send all correspondence to: V. Foulon, PharmD, PhD, KU Leuven, Department of Pharmaceutical and Pharmacological Sciences – Clinical Pharmacology and Pharmacotherapy, Herestraat 49, bus 521, 3000 Leuven, Belgium, tel: + 32 (0)16 32 34 64, email: veerle.foulon@kuleuven.be.
Acknowledgements: With the contribution of CMP Vlaanderen, Heilig Hart Ziekenhuis Lier, AZ Groeninge, UZ Gent, UZA and Centres Hospitaliers Jolimont. We are grateful to all patients and health care professionals who participated in this research.
Conflict of interest: Takeda funded this work. The research team of KU Leuven/UGent conducted this study independently, according to an agreement. There was no interference of Takeda in the course of the study.
Composition expert panels participating in the co-design process.
FIGURE 1.
Summary of the 2-phase co-design development of the PARTNER model and tools.
FIGURE 2.
PARTNER model for SDM.
References
1. Wilke T, et al. Treatment of relapsed refractory multiple myeloma: which new PI-based combination treatments do patients prefer? Patient Prefer Adherence. 2018;12:2387–96.
2. Cook G, et al. A question of class: Treatment options for patients with relapsed and/or refractory multiple myeloma. Crit Rev Oncol Hematol. 2018;121:74–89.
3. Moreau P, et al. Global Approaches in Myeloma: Critical Trials That May Change Practice. Am Soc Clin Oncol Educ Book. 2018;38:656–61.
4. Kumar SK, et al. NCCN Guidelines Insights: Multiple Myeloma, Version 3.2018. J Natl Compr Canc Netw. 2018;16(1):11–20.
5. Covvey JR, et al. Barriers and facilitators to shared decision-making in oncology: a systematic review of the literature. Support Care Cancer. 2019;27(5):1613–37.
6. LeBlanc TW, et al. Review of the patient-centred communication landscape in multiple myeloma and other hematologic malignancies. Patient Educ Couns. 2019;102(9):1602–12.
7. Tariman JD, et al. Top Information Need Priorities of Older Adults Newly Diagnosed With Active Myeloma. J Adv Pract Oncol. 2015;6(1):14–21.
8. Kane HL, et al. Implementing and evaluating shared decision making in oncology practice. CA Cancer J Clin. 2014;64(6):377–88.
9. Rood JA, et al. Perceived need for information among patients with a haematological malignancy: associations with information satisfaction and treatment decision-making preferences. Hematol Oncol. 2015;33(2):85–98.
10. Tariman JD, et al. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–51.
11. Gilligan T, et al. Patient-Clinician Communication: American Society of Clinical Oncology Consensus Guideline. J Clin Oncol. 2017;35(31):3618–32.
12. Légaré F, et al. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff (Millwood). 2013;32(2):276–84.
13. Elwyn G, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–7.
14. Charles C, et al. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–92.
15. Legare F, et al. Interventions for improving the adoption of shared decision making by healthcare professionals. Cochrane Database Syst Rev. 2014(9): CD006732.
16. Weston WW. Informed and shared decision-making: the crux of patient-centred care. CMAJ. 2001;165(4):438–9.
17. Barratt A. Evidence Based Medicine and Shared Decision Making: the challenge of getting both evidence and preferences into health care. Patient Educ Couns. 2008;73(3):407–12.
18. Vandvik PO, et al. Creating clinical practice guidelines we can trust, use, and share: a new era is imminent. Chest. 2013;144(2):381–9.
19. Elwyn G, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891.
20. McLawhorn VC, et al. Integrating a Question Prompt List on an Inpatient Oncology Unit to Increase Prognostic Awareness. Clin J Oncol Nurs. 2016;20(4):385–90.
21. kanker.nl. Vragen uit de app Gesprekshulp bij kanker [Available from: https://www.kanker.nl/gesprekshulp/vragen-voor-het-gesprek].
22. Van Hecke A, et al. Het Digitaal Onco Platform (DOP): op weg naar verdieping en verbreding. Optimalisatie en implementatie van het eHealth platform voor kankerpatiënten. Stichting Tegen Kanker, Social Grant. 2015.
23. Brandes K, et al. Advanced cancer patients' and caregivers' use of a Question Prompt List. Patient Educ Couns. 2014;97(1):30–7.
24. Chhabra KR, et al. Physician communication styles in initial consultations for hematological cancer. Patient Educ Couns. 2013;93(3):573–8.
25. Paladino J, et al. Patient and clinician experience of a serious illness conversation guide in oncology: A descriptive analysis. Cancer Medicine. 2020; 9(13):4550–60.
26. Bernacki RE, et al. Communication About Serious Illness Care Goals. JAMA Internal Medicine. 2014;174(12):1994.
27. Morgans AK,et al. Confronting Therapeutic Failure: A Conversation Guide. The Oncologist. 2015;20(8):946–51.
28. Leblanc TW, et al. Review of the patient-centred communication landscape in multiple myeloma and other hematologic malignancies. Patient Educ Couns. 2019;102(9):1602–12.
29. Kinnaer L-M, et al. Key elements for the education and counselling of patients treated with oral anticancer drugs. Eur J Oncol Nurs. 2019;41:173–94.
30. Lomas J. Diffusion, dissemination, and implementation: who should do what? Ann N Y Acad Sci. 1993;703:226–35; discussion 35–7.
31. Pearson A, Wiechula R, Court A, et al. The JBI model of evidence-based healthcare. Int J Evid Based Healthc. 2005;3(8):207–15.
32. Clayton JM, et al. Randomized controlled trial of a prompt list to help advanced cancer patients and their caregivers to ask questions about prognosis and end-of-life care. J Clin Oncol. 2007;25(6):715–23.
33. Rodenbach RA, et al. Promoting End-of-Life Discussions in Advanced Cancer: Effects of Patient Coaching and Question Prompt Lists. J Clin Oncol. 2017;35(8):842–51.
34. Keinki C, et al. Effect of question prompt lists for cancer patients on communication and mental health outcomes—A systematic review. Patient Educ Couns. 2021.
35. Bruera E, et al. Breast cancer patient perception of the helpfulness of a prompt sheet versus a general information sheet during outpatient consultation: a randomized, controlled trial. J Pain Symptom Manage. 2003;25(5):412–9.
36. Smets EM, et al. Addressing patients' information needs: a first evaluation of a question prompt sheet in the pretreatment consultation for patients with esophageal cancer. Dis Esophagus. 2012;25(6):512–9.
37. Brown RF, et al. Promoting patient participation and shortening cancer consultations: a randomised trial. Br J Cancer. 2001;85(9):1273–9.
38. Onel E, et al. Assessment of the Feasibility and Impact of Shared Decision Making in Prostate Cancer. Urology. 1998;51(1):63–6.
39. Ross L, et al. Applicability of a video intervention to increase informed decision making for prostate-specific antigen testing. J Natl Med Assoc.2010;102(3):228–36.
40. Frosch DL, et al. A randomized controlled trial comparing internet and video to facilitate patient education for men considering the prostate specific antigen test. J Gen Intern Med. 2003;18(10):781–7.
41. Tai-Seale M, et al. Enhancing Shared Decision Making Through Carefully Designed Interventions That Target Patient And Provider Behavior. Health Aff (Millwood). 2016;35(4):605–12.
42. Kinnaer LM, et al. Collaborative network to take responsibility for oral anticancer therapy (CONTACT): Study-protocol investigating the impact of a care pathway. J Adv Nurs. 2019;75(12):3726–39.
Please send all correspondence to: V. Foulon, PharmD, PhD, KU Leuven, Department of Pharmaceutical and Pharmacological Sciences – Clinical Pharmacology and Pharmacotherapy, Herestraat 49, bus 521, 3000 Leuven, Belgium, tel: + 32 (0)16 32 34 64, email: veerle.foulon@kuleuven.be.
Acknowledgements: With the contribution of CMP Vlaanderen, Heilig Hart Ziekenhuis Lier, AZ Groeninge, UZ Gent, UZA and Centres Hospitaliers Jolimont. We are grateful to all patients and health care professionals who participated in this research.
Conflict of interest: Takeda funded this work. The research team of KU Leuven/UGent conducted this study independently, according to an agreement. There was no interference of Takeda in the course of the study.